Written by – Ogunfeitimi Iyanuoluwa Faith
Health policy is not Nigeria’s challenge; the real problem is the implementation gap. A country with well-crafted health policies but no meaningful implementation is essentially living in what many young Nigerians casually call “delulu”, also known as “delusion.”
One of the major barriers to effective policy implementation in Nigeria is the presence of deep systemic constraints. Policies are often developed by one administration, but there is rarely a seamless transition of ideas to the next. A new government comes in, discards the old initiatives, and begins an entirely new set of programmes that may also be abandoned once that administration ends. This cycle repeats itself, and the nation continues to move in circles.
It is unfortunate that health policymakers spend countless hours crafting evidence-based policies, engaging stakeholders, and pushing for adoption, only for these policies to remain on paper because of political turnover, institutional weaknesses, and competing priorities.
From my perspective, what Nigeria needs right now is not another set of recommendations or yet another policy document. What we need is honest introspection and a commitment to addressing the systemic barriers that have held back national development for decades.
Over the past 15 years, Nigeria has attempted many health reforms that were well-designed, promising, yet their implementation remains stalled.
Nigeria, the giant of Africa, is resource-rich and ranks among the world’s 13th-largest oil producers, yet when it comes to the health sector, we are the second-lowest globally. This reflects our systemic gaps more than our resource limitations.
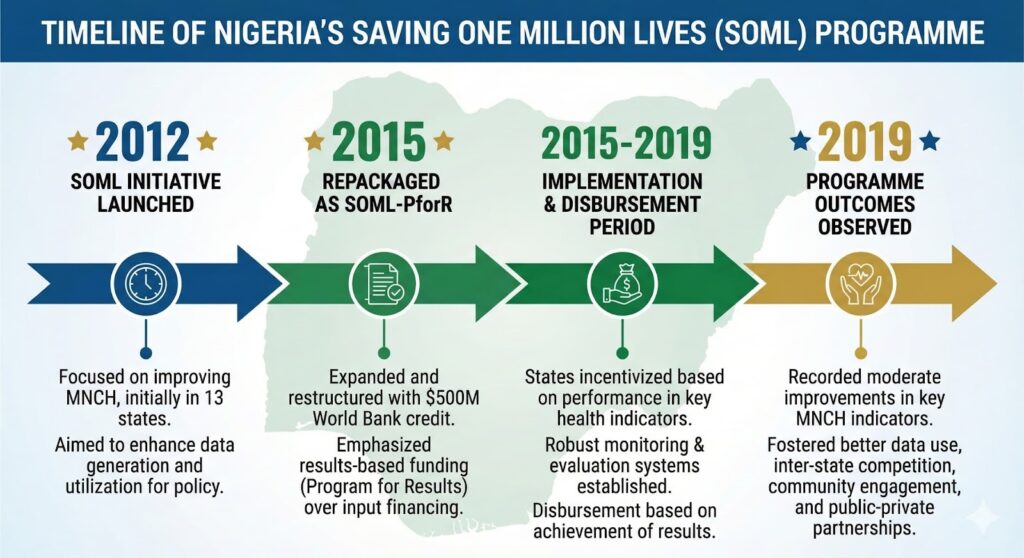
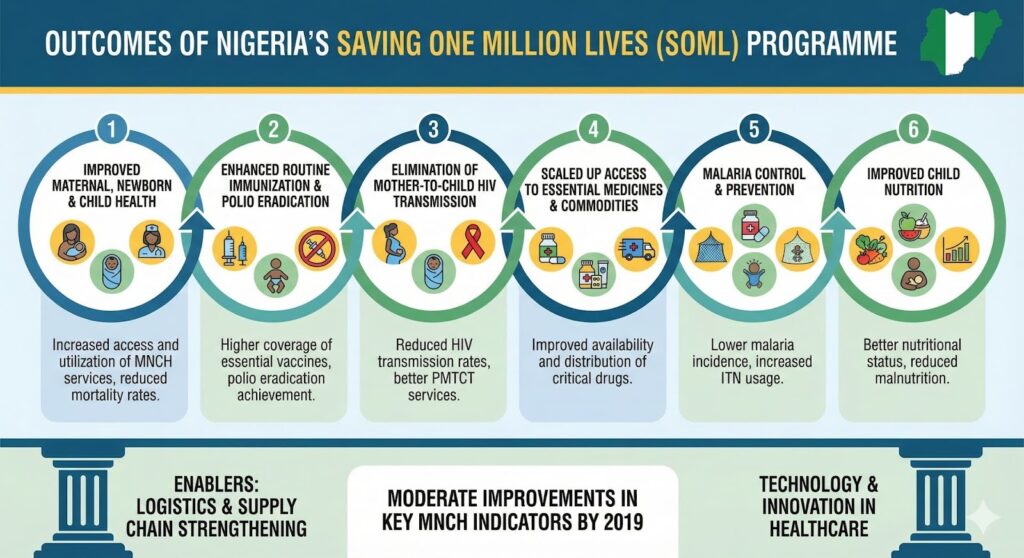
A clear example is the Saving One Million Lives (SOML) initiative developed under Minister of State for Health Mohammed Pate during President Goodluck Jonathan’s administration. Once Pate left the Federal Ministry of Health (FMOH) in 2013, the implementation took a back seat. This is the Nigerian cycle: the arrival of a new government often means an abrupt halt to existing programmes in favour of brand-new ones. Some of the problems facing the nation are not new, the communities are not new, and the system remains largely unchanged.
Research has shown this pattern clearly. The Subsidy Reinvestment and Empowerment Programme – Maternal and Child Health (SURE-P MCH) component was abruptly discontinued simply because it was perceived as “Goodluck Jonathan’s project.” As one interviewee put it, “SOML became an orphan. No one was owning it. There was no appropriation for it.” Yet the original goal of SOML was straightforward: reduce preventable mortality by scaling proven interventions.
Another instance is the National Health Act (NHA). The bill passed the Federal Executive Council and the Senate in 2007, but because it did not pass the House before President Obasanjo left office, it was never adopted. A similar bill successfully passed both legislative chambers in 2011, but it was not signed by President Jonathan. Analysts have noted that despite strong support from civil society organizations, the bill lacked committed champions within government. Donor-funded groups like the Health Reform Foundation of Nigeria (HERFON) could only push so far without internal government leadership.
It was only in 2014, near another election, that the NHA was finally signed. Even then, implementation continued to face opposition, delays, and political resistance. For example, although over 7,000 facilities have now received Basic Health Care Provision Fund (BHCPF) disbursements, the scale of progress remains modest compared to national needs. Programmes collapsed or stalled due to political transitions: SOML lost momentum after Minister Pate left; SURE-P was discontinued after President Jonathan was voted out; and BHCPF slowed significantly when Minister Adewole left office in 2019.
This pattern highlights a painful truth: programmes that depend heavily on individual champions rather than institutional strength are unlikely to survive political turnover.
A Leadership Thought
To address these systemic issues, we must begin from within. I am not waiting to “become” a healthcare leader in the future; I am a healthcare leader now. And leadership, to me, means cultivating a culture where the baton is passed responsibly, not dropped. Tenure transitions should represent continuity, not the abandonment of progress.
Nigeria does not suffer from a shortage of ideas. We suffer from an inability to sustain them. Until we build systems that outlive individuals, governments, and political cycles, our health policies will remain beautifully written but poorly executed.
Leadership at every level, whether institutional, governmental, organizational, or personal must redefine progress as continuity , not constant reinvention. That’s the mindset shift Nigeria needs if we are truly ready for a long term national growth and healthcare system strengthening.
List of Abbreviations in graphics
- MNCH – Maternal, New-born and Child Health.
- PMTCT – Prevention of Mother-To-Child Transmission.
- ITN – Insecticide-Treated Net.
Acknowledgement/References
- Kevin Croke, Osondu Ogbuoji, Health reform in Nigeria: the politics of primary health care and universal health coverage, Health Policy and Planning, Volume 39, Issue 1, January 2024, Pages 22–31, https://doi.org/10.1093/heapol/czad107
- Isaac F. Adewole and Olusoji Adeyi, Saving one million lives programme for results and implementation in Nigeria: A report, African Journal of Reproductive Health, 22 Nov 2022